
Data from a specialist Australasian registry suggests the proportion of patients with Crohn’s disease or ulcerative colitis was higher in overweight and obese individuals.
Australian experts are calling for more detailed anthropometric screening in patients with IBD.
Inflammatory bowel disease (IBD) – specifically Crohn’s disease (CD) and ulcerative colitis (UC) – and obesity are both becoming more prevalent in Australia and New Zealand. While IBD and obesity were originally thought not be related, there is a small amount of evidence to suggest the two are somehow linked.
Now, a new research study has reported the prevalence of obesity in a large cohort of Australasian adults with IBD for the first time.
“Our findings provide the first Australasian data on this critical issue and carry significant implications for clinical management and health service planning for IBD in Australia, reflecting an urgent need for a paradigm shift in the routine management of IBD,” the researchers wrote in the Internal Medicine Journal.
“The focus can no longer be solely on managing IBD; clinicians must now proactively screen and manage obesity as a metabolic comorbidity that can equally affect IBD course.”
The Australian researchers used data from the Crohn’s Colitis Cure (CCCure) registry, an IBD-specific electronic medical record used by hospital-based IBD specialist clinics across Australia and New Zealand. Adult patients (aged 18 years and older) with a confirmed IBD diagnosis who had a documented clinical encounter in the 14 months prior to May 2025 were included. Patients with missing height and/or weight data (required to calculate BMI) were excluded.
There were 7134 individuals with IBD included in the final sample, with 3909 (54.8%) diagnosed with CD and 3225 (45.2%) diagnosed with UC. There was equal gender representation, with 3552 participants (49.8%) identifying as female. The median age was 44.7 years, and the median duration of disease was 13.9 years.
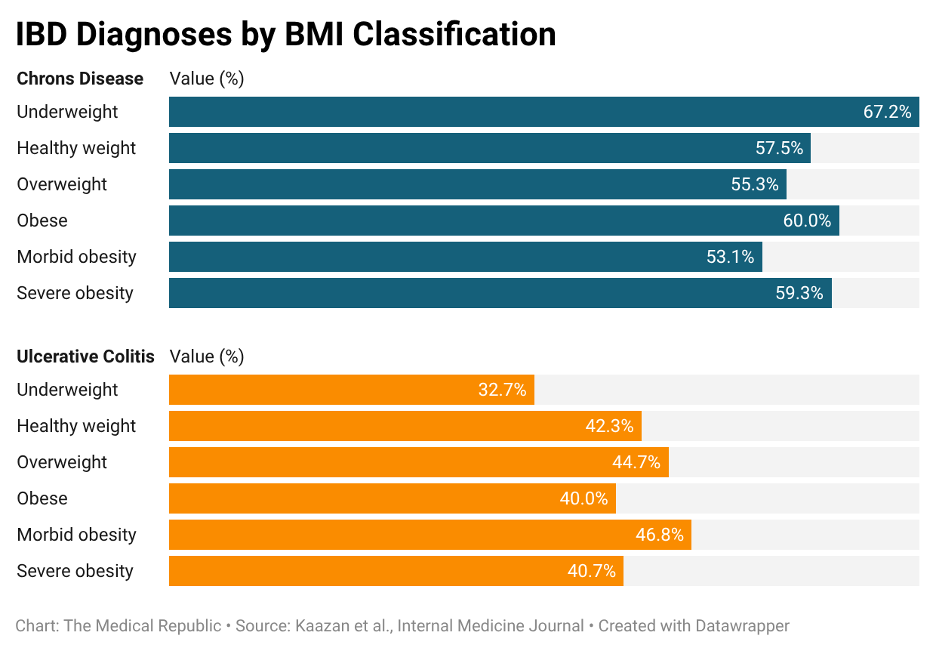
The average BMI across all patients was 26.6kg/m2. Based on the World Health Organization’s BMI classification, 2300 participants (32.2%) were overweight (a BMI between 25.0 and 29.9kg/m2) and a further 1654 (23.2%) were obese (BMI ≥30kg/m2). The proportion of overweight and obese participants in the current study was similar to that of the broader Australian population, with the Australian Bureau of Statistics reporting 65.8% of adults were overweight or obese in 2022.
Obesity was more prevalent in people with CD (24.7%) compared to people with UC (21.3%), a finding that remained when patients were grouped according to their BMI classification. The proportion of patients with IBD was higher in overweight and obese patients compared to those with a healthy weight.
An increase in BMI was also associated with an increase in the proportion of patients with major cardiometabolic comorbidities (i.e., diabetes and metabolic dysfunction-associated fatty liver disease) and the proportion of patients who had used a GLP-1 receptor agonist.
The researchers claimed that the results “challenge the historical perception of IBD as a predominantly wasting disease and position obesity as a major comorbidity in the contemporary Australasian IBD management landscape”.
Related

“Historically, the clinical picture in IBD has been inextricably linked to malnutrition with an underweight phenotype, which was associated with poor clinical outcomes. However, over the past two decades, there has been a growing body of evidence that suggests the prevalence of overweight and obesity within IBD populations has risen dramatically,” they said.
“A key finding is the strong association between BMI and IBD subtype… Interestingly, there is a higher proportion of CD in patients in all obesity categories compared with UC. These data align with large cohort studies suggesting an association between obesity and CD.”
While there is some evidence of a common underlying mechanism between obesity and IBD, it’s far from concrete, according to the researchers.
“It is plausible that factors characteristic of a ‘Western’ lifestyle, such as diets high in ultra-processed foods, saturated fats and refined sugars, alongside reduced physical activity, are known to promote gut dysbiosis, a state of microbial imbalance implicated in the pathogenesis of both obesity and IBD,” they said.
“A pathobiological linkage between the two conditions is [also] plausible through common environmental risk factors such as high-fat low-fibre diet, intestinal microbiome alterations and a metabolically active visceral adipose tissue, but epidemiological studies associating this linkage are limited, and more robust longitudinal prospective studies are needed.”
The researchers called for additional biometric data to be collected in the clinic to assist with screening and early intervention, a pertinent point given over 2500 individuals were excluded from the current study due to missing height or weight data.
“We suggest routine implementation of waist circumference (an indirect measure of visceral adiposity) in day-to-day IBD practice, as it may be a better predictor of fat mass distribution, and consequently, the risk of obesity-related complications,” they wrote.
“We also call all IBD clinicians to document anthropometrics such as height, weight and waist circumference for every patient with IBD to optimise care. Muscle health should equally be assessed in patients with IBD at routine intervals, as there is a growing body of evidence that suggests increasing obesity rates coincide with sarcopenia, which is associated with poor clinical outcomes.”
Further information about the CCCure registry is available via the Crohn’s Colitis Cure website.
